A 26 year old male patient presented with chronic diarrhoea
Hi, I am S.Sathwika Reddy , 3rd Sem Medical Student.This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.”
I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
CHIEF COMPLAINTS
Chronic diarrhoea since 20 days
HISTORY OF PRESENTING ILLNESS
Patient was apparently asymptomatic 2 months ago, then he developed bilateral flank pain. He also developed loose stools which were insidious in onset with 4-5 episodes per day (10 days liquid consistency, 10 days hard consistency). He was suffering from generalised body weakness since 3 years and is not associated with fever, nausea and vomiting.
HISTORY OF PAST ILLNESS
The patient is a known case of diabetes mellitus since 3 years.
He is on irregular medication and stopped taking insulin 7 months ago.
He is also a known case of polio.
PERSONAL HISTORY
Unmarried
Diet: mixed
Appetite:normal
Sleep: normal
Bowel: regular
Bladder: increased frequency of micturition
No known allergies
Addictions: alcohol since 5 years (daily intake- quarter)
FAMILY HISTORY
No significant family history
GENERAL EXAMINATION
Patient was conscious, coherent and cooperative.
Pallor is absent
Icterus is absent. No cyanosis, clubbing koilonychia, lymphadenopathy.
Pedal oedema absent.
VITALS:
Pulse: 90 bpm
BP: 110/70 mm of Hg
Temperature: 98.4°F
RR: 18/ min
SPO2: 96%
SYSTEMIC EXAMINATION:
Cardiovascular system:
No thrills
No murmur
Respiratory system:
Dyspnea is absent.
Wheeze: no
Abdomen:
Shape : scaphoid
No tenderness
No palpable mass
CNS:
Conscious
Normal speech
Gait - normal
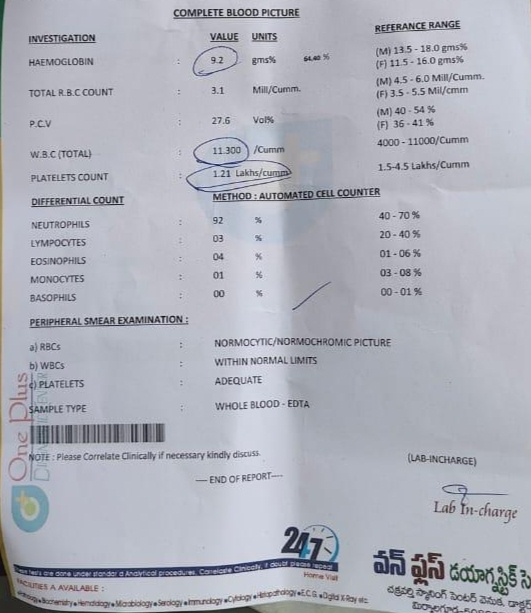
INVESTIGATIONS:
Complete blood picture

TPR GRAPH

ECG

Acute pancreatitis